There are two reasons why you might be given antibiotics during labour:
1) Known risk of an infection
Antibiotics in labour will be recommended if there is an increased risk of infection to the baby by bacterium called Group B Streptococcus (GBS). This could be indicated in labour if:
a) results in your current or previous pregnancy have detected GBS in vaginal or urine testing; or
b) labour starts prior to 37 weeks and is associated with rupture of membranes prior to the onset of labour.
The team will check your allergies and available results to determine which antibiotics to give you until your baby is born. When antibiotics are administered for this indication only, you will be able to walk around in labour.
2) Signs of a possible infection
Infection in labour may be suspected based on symptoms like fever, or signs like a higher than expected heart rate in you or baby in the womb.Infection can occur in any part of your body. If we can’t identify where the infection is, we work on the assumption that it could be in the womb, and this may be difficult to confirm until at least a few days later.Untreated infection can sometimes spread to the blood and if not treated it may have serious consequences. Given the risk that an infection may pose, the medical team will undertake a detailed assessment of you and your baby. They will conduct a range of tests on you to help establish the type of infection. This will include blood tests, urine tests and vaginal swabs. The tests include full blood count, C-reactive protein (CRP), blood/urinary/vaginal culture and sensitivity. The team will recommend starting antibiotics through a cannula (a very fine, flexible plastic tube) directly into your vein.You will need to be monitored closely and this will involve continuous monitoring of you and the baby, which may limit you from walking around in labour. We will continue to support your birth preferences as best as possible and discuss all options and recommendations so that you can make informed choices about your care. We will help you adopt positions that are comfortable for you and that are known to support vaginal births.Some of the blood results will be available within a few hours and some tests (microbiological cultures and sensitivity) may take up to 3 days.Your team will continue to monitor you and your baby closely through your labour and will keep you informed of their findings and recommendations. You are encouraged to ask any questions or share concerns you may have.
What will happen after the birth?
1) Known risk of an infection
If you received antibiotics in labour only because of the known risk of GBS infection, this will be stopped at the time of the birth. For 12-24 hours after the birth, your team will monitor you and the baby for anything concerning, including signs of infection. The monitoring aims to identify early warning symptoms and signs. For the baby, this will include overall assessment and regular measurement of heart rate, respiratory rate, colour, temperature and feeding. The baby will stay with their mothers on the postnatal ward.
2) Signs of a possible infection
Your antibiotics will be continued through the cannula until your temperature has been normal for at least 24 hours after the birth, you feel well and the infection results indicate an improvement.Based on your recovery and test results, you may need to continue the antibiotic course as tablets. The total duration of antibiotics can vary but they will be safe to take if you are breastfeeding.If you have a urinary infection, you will need to repeat a urine test (culture and sensitivity) a week after you complete your antibiotics course to make sure the infection has been treated fully.
Supporting your partner during labour and birth can be a rewarding and bonding experience for both of you. Use the Personalised Birth Preferences plan in the app to help you think about both of your needs and choices for labour and birth.Staying well-hydrated and nourished during the labour will help you to stay alert, so come prepared with non-perishable snacks and drinks. It is also okay to take a break occasionally, especially if labour is long. Chat about this with your partner before labour so everyone’s expectations can be met.If you have helped to pack the hospital bag, you will know where to find a hat and nappy for your newborn baby, as these are the first things the midwife will ask you for.Depending on hospital policy it may be possible to have more than one birth partner during labour. It is wise to check with your midwife ahead of time.
Sometimes babies are born so early or so unwell it is very hard for them to survive despite having intensive care. This will be a very difficult time for you and your family. Your baby will have fought so hard to have met you and spend time with you since their birth.Whilst your baby is still alive, you may wish to make memories with them such as making prints of their hands and feet, taking photos and videos of you all together, introducing them to siblings and family they may not have met yet, reading them your favourite books and having a ceremony to celebrate their life. The neonatal team helping you to care for your baby will be able to assist you with all these things and any other requests you may have.
End of life care for your baby
If the neonatal team has spoken to you about your baby dying, they may start to change the focus of their care from active care to focusing more on maximising their comfort. This may involve doing fewer painful procedures on your baby or starting your baby on some medicines to keep your baby comfortable.The team will discuss with you, whenever possible, about where you would like to be with your baby when they stop receiving active treatment and transition to receiving comfort-focused care. This is usually in hospital, but may be in a hospice, or even at home. The neonatal staff will support in making these decisions. The neonatal team may also introduce you to the palliative care team, who are experts in caring for babies with life-limiting conditions.The team will also discuss with you whether you would like your baby to have a postmortem examination to find out more about the problems that have made your baby so ill. There are also some instances where the coroner may make this decision.
After your baby has died on a neonatal ward
The neonatal unit staff will support you to be able to provide care for your baby around the time of death. They will issue you with a death certificate and provide you with all the information you need about registering your baby’s death. You will be offered a bereavement appointment to talk about your baby’s care a few weeks after their death. A bereavement nurse will be in regular contact with you too.
Transitional care is when you and your baby stay together in hospital with support from the hospital staff. It means that your baby is well enough to stay with you either on the postnatal ward or a room near the neonatal unit. You will be in hospital with your baby. Common reasons for a baby requiring transitional care include:
babies born early between 33 and 35 weeks
babies with jaundice requiring treatment
babies needing antibiotic treatment
babies requiring extra support with their feeding.
Your baby will be reviewed regularly by one of the neonatal doctors or nurses whilst they are in transitional care and the treatment plan will be discussed with you.Some babies may need more care than can be provided on the postnatal ward or in transitional care and they are admitted to the neonatal unit. The main reasons for a baby to be admitted are that they are born prematurely, have a low birth weight or have a specific medical condition which needs treatment in hospital. When your baby is admitted one of the neonatal team will be able to update you on your baby’s condition and progress. You will be able to visit your baby at any time on the neonatal unit.Neonatal care is organised across the country in regional networks of neonatal units. The units provide different levels of care to babies depending on how early or unwell they are.If there is a suspicion that your baby will need a higher level of care than the hospital you are in can provide, you may be moved to a different hospital before your baby is born. This is called “In-utero transfer” (your baby is still in your uterus). If the move happens after your baby is born because they have arrived earlier than expected or are unwell, this is called “ex-utero transfer”. The neonatal team will always ensure that you and your baby are not separated for any longer than is necessary.There are three types of neonatal unit, which provide different levels of care depending on what your baby needs. These are:Special Care Baby Unit (SCBU): the care provided here is usually for babies born after 32 weeks gestation, or babies who only require a low level of support, such as some oxygen or a drip for a short time.Local neonatal unit (LNU): the level of care provided here is for babies who need more support than those in a SCBU, as they are born betwen 28 and 32 weeks gestation or are unwell and may require a short period of intensi ve care or high dependency care, including help with breathing.Neonatal Intensive Care Unit (NICU): this is for babies born earlier than 28 weeks gestation or those who are very unwell for other reasons. The NICU can look after babies of all gestations and is sometime called a “tertiary” unit. Some of these units specialise in surgery for baby or other types of highly specialised care. If your baby needs to be in a NICU, they will usually need to be on a breathing machine (ventilator).If your baby needs to be transferred to another hospital after birth, the Neonatal Transport Service will come and look after your baby and transfer them to the new hospital. If you are well enough to be discharged you will be able to meet your baby at the new hospital. If you are not well enough suitable arrangements will be made for your ongoing care.When your baby is well enough they will be moved back to the hospital that is closer to your home. This allows you and your baby to get to know the team who will be looking after them once they are discharged home.
If you have had a healthy pregnancy without complication and haven’t gone into labour by 41 weeks you will have a routine appointment with your midwife to discuss the next steps.
What happens at your 41 week appointment?
You will be offered a membrane sweep, which is an internal examination of the cervix. During this examination your midwife will insert the tip of her finger into your cervix and sweep around the bag of membranes that cover your baby’s head. This has been shown to release hormones that may encourage labour to start within 24 hours. Sometimes the cervix isn’t yet open, and a sweep isn’t possible. You may be invited to return for more sweeps.Your midwife will also offer you a date to have your labour induced. This is normally recommended by 41 weeks and three, four or five days (depending on your maternity units guidelines and availability). Some maternity units are able to offer complementary therapy to encourage labour to start naturally. Ask your midwife about this.
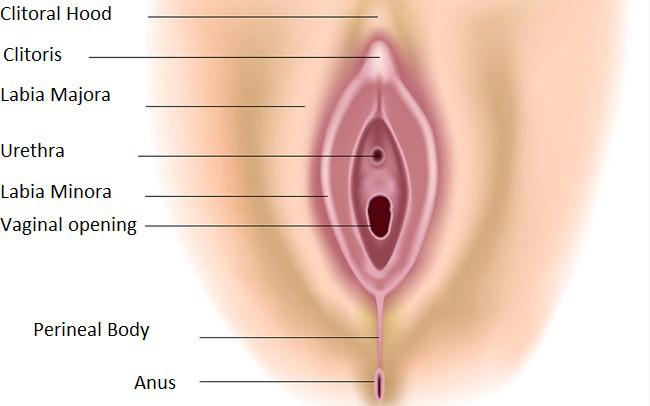
When your baby is born, his or her head stretches the opening of the vagina. The skin inside and surrounding the vagina will often stretch well to allow your baby to be born, however during this process it is common for women to sustain a tear to the inside of the vagina and/or the skin inside the vagina or both – which may require stitches. The stitches used will always be dissolvable and should not need to be removed.First degree tears These affect the skin of the perineum/vagina. Some of these tears require stitches and some may heal well without stitches. Your midwife will advise you on this after birth.Second degree tears These affect the skin and muscle of the perineum/vagina. Most of these tears require stitches to assist with healing.Third and fourth degree tears These affect the skin and muscle of the perineum/vagina, as well as some of the structures associated with the anal sphincter. These tears require a repair by an obstetric doctor, under surgical conditions to repair them.Labial tears These occur to the labia minora and will often require stitches to aid healing. Your midwife will advise you on this after birth.Episiotomies These are sustained during the birth, when your doctor or midwife makes a cut to facilitate the birth of your baby. These are similar to second degree tears and will require stitches.
After the birth, the midwife will prepare two infant identity bands. Each band will include the mum’s surname and the hospital number. Details will be checked with the mum and/or partner against the mum’s printed patient identity band before placing it on the baby. A unique NHS number and hospital number will be generated for your baby shortly after birth. The NHS number will remain with your baby throughout their life.


 There are two reasons why you might be given antibiotics during labour:
There are two reasons why you might be given antibiotics during labour: