
Recovery from vaginal or assisted birth

 Once you are admitted to the postnatal ward or discharged home from hospital to the care of the community midwife, you can expect that your body will need some time to recover from the birth. Midwives, maternity support workers or nurses may be involved in your care and will carry out routine checks to ensure that you are well. This will include a regular top to toe physical check, including inspection of sutures (stitches).
If you have had a vaginal birth you will be offered pain relief. Read “Commonly used medicines” to find out what painkillers are routinely offered. Read “After pains” and “Perineal after-care” which explains how you can help yourself if you are experiencing after pains or if you have had an episiotomy (cut) or a perineal tear. If you have had an assisted delivery you may need to have a urinary catheter for a few hours. Read “Passing urine” for more information.
It is important to eat well and drink plenty of fluids to promote health and wellbeing after any type of birth.
Once you are admitted to the postnatal ward or discharged home from hospital to the care of the community midwife, you can expect that your body will need some time to recover from the birth. Midwives, maternity support workers or nurses may be involved in your care and will carry out routine checks to ensure that you are well. This will include a regular top to toe physical check, including inspection of sutures (stitches).
If you have had a vaginal birth you will be offered pain relief. Read “Commonly used medicines” to find out what painkillers are routinely offered. Read “After pains” and “Perineal after-care” which explains how you can help yourself if you are experiencing after pains or if you have had an episiotomy (cut) or a perineal tear. If you have had an assisted delivery you may need to have a urinary catheter for a few hours. Read “Passing urine” for more information.
It is important to eat well and drink plenty of fluids to promote health and wellbeing after any type of birth.



 Feeling lonely and isolated after the birth of a baby is not uncommon for new parents, particularly for those who may not have close family nearby for companionship and support.
Read the article in Emma’s diary to find out what you can do if you feel lonely.
Feeling lonely and isolated after the birth of a baby is not uncommon for new parents, particularly for those who may not have close family nearby for companionship and support.
Read the article in Emma’s diary to find out what you can do if you feel lonely.

 Having a premature baby is the beginning of a long and emotional journey towards going home. It can be a very stressful time for your whole family. A premature baby’s development happens in the same order as it would have happened in your womb. When your baby reaches certain health, growth and development milestones, you’ll be able to take them.
All babies are different, and their behaviour and development are different too. In premature babies, the differences have to do with how premature they were when they were born.
Below are some changes that you can expect and watch out for in your premature baby and what you can do to help their development.
Having a premature baby is the beginning of a long and emotional journey towards going home. It can be a very stressful time for your whole family. A premature baby’s development happens in the same order as it would have happened in your womb. When your baby reaches certain health, growth and development milestones, you’ll be able to take them.
All babies are different, and their behaviour and development are different too. In premature babies, the differences have to do with how premature they were when they were born.
Below are some changes that you can expect and watch out for in your premature baby and what you can do to help their development.
|
23 to 27 weeks gestation |
|
| Weeks of gestation/Cues | What you can do to help |
|---|---|
| 23 weeks: Eyes are closed. Little movement. | Ask your baby’s nurse to show you how you can touch your baby. Familiarise yourself with the BLISS family handbook. |
| 24 weeks: Your baby’s skin is very thin and transparent. | Talk quietly to your baby as they can hear you. |
| 25 weeks: Your baby’s body is lean with no fat. His/hers arms and legs are limp. Your baby doesn’t yet have good muscle tone. | Ask your baby’s nurse about how to hold and position your baby. Leave a small piece of cloth that smells of you with your baby. |
| 26 weeks: Your baby’s eyes will start to open but they can’t focus yet. Your baby will sleep a lot. The breath triggering part of your baby’s brain hasn’t fully developed yet, so pauses between breaths are common. | Keep the lights as dim as possible. Shield your baby’s eyes from bright light to enable your baby to try and open their eyes. |
| 27 weeks: Your baby may startle at loud noises. | Avoid sudden noises. Remember positioning. |
|
28 to 32 weeks gestation |
|
| Weeks of gestation/Cues | What you can do to help |
|---|---|
| 28 weeks: Your baby’s movements may be jerky and jittery. Their hand grasp and sucking reflexes appear but these will be weak. | Ask the nurse about skin to skin contact (kangaroo mother care). Let your baby gently hold your finger. Your baby may take a non-nutritive tool. |
| 29 weeks: The ability to hear and smell will allow your baby to recognise you. | Talk softly to your baby when you visit. You may like to read short stories, nursery rhymes or sing to your baby. |
| 30 weeks: Your baby has periods of alertness and sleep Your baby may recognise your face now. | Try to observe the periods of alertness in your baby, to allow them to look at you and interact |
| 31 weeks: Your baby may be able to keep his/hers eyes open wide for a time. | Move your face back and forth slowly and your baby may follow you and your eyes. |
| 32 weeks: Your baby will be more interested in sucking and may appear to suck the feeding tube. | Offer a non-nutritive feed with tube feeds. Speak to your baby’s nurse about cup feeds if appropriate. |
|
33 to 37 weeks gestation |
|
| Weeks of gestation/Cues | What you can do to help |
|---|---|
| 33 weeks: There are clear sleep and awake cycles. Your baby will be moving around in the cot and incubator a lot. | Provide a calm environment around feeding time to enable your baby to focus on sucking, swallowing and breathing. |
| 34 weeks: Your baby may be sucking on hands and non-nutritive tools. | Offer the breast, or start using your own bottles and teats. Hold your baby still rather than rocking them to enable them to gradually become accustomed to position changes. |
| 35 weeks: Your baby may wake up when hungry, may cry with a wet or dirty nappy. | Allow your baby to gaze at your face. Talk or sing in a soft voice whilst your baby is in light sleep. |
| 36 weeks: Your baby may have a more consistent sleep/wake cycle. Your baby may want to be held and cuddled more. | Parents’ voices, smells and faces are very important. |
| 37 weeks: Your baby should be gaining more weight and has fuller cheeks. | Spend as much time as you can with your baby. If you haven’t talked about or arranged an overnight stay, this is a good time to book it. Ask the team about resuscitation training. |

 Oral thrush is a common fungal infection in the mouth. It can be easily and quickly treated if it doesn’t clear up on its own.
Oral thrush is a common fungal infection in the mouth. It can be easily and quickly treated if it doesn’t clear up on its own.

 Eating healthily after the birth of your baby is as important as it was during pregnancy. Eating a balanced diet with plenty of clear fluids helps your body to recover. Speak to your midwife, health visitor, infant feeding specialist or GP if you have specific concerns relating to weight loss, diabetes or breastfeeding.
Eating healthily after the birth of your baby is as important as it was during pregnancy. Eating a balanced diet with plenty of clear fluids helps your body to recover. Speak to your midwife, health visitor, infant feeding specialist or GP if you have specific concerns relating to weight loss, diabetes or breastfeeding.

 Additional resources are available to help you with finances, housing, infant feeding, peer suppport, social activities in your local council area. Go to your council website to discover these and more resources.
Additional resources are available to help you with finances, housing, infant feeding, peer suppport, social activities in your local council area. Go to your council website to discover these and more resources.
 Paediatricians or neonatologists are doctors specialising in the care of newborn babies and children. They will be involved in your care if early (premature) delivery is anticipated or if there are likely to be concerns about the health of your baby during or after the birth.
Paediatricians or neonatologists are doctors specialising in the care of newborn babies and children. They will be involved in your care if early (premature) delivery is anticipated or if there are likely to be concerns about the health of your baby during or after the birth. 
 During pregnancy, the body naturally retains more fluid, and swelling of the hands is common. If some of this fluid is localised to the carpal tunnel, this leads to pressure on the median nerve causing the symptoms of CTS. Up to 62% of pregnant women develop CTS. These symptoms are also common after the birth.
During pregnancy, the body naturally retains more fluid, and swelling of the hands is common. If some of this fluid is localised to the carpal tunnel, this leads to pressure on the median nerve causing the symptoms of CTS. Up to 62% of pregnant women develop CTS. These symptoms are also common after the birth.
 2. Hand squeeze. Make a release a fist (this can be done with your hands elevated). You could also squeeze a stress ball:
2. Hand squeeze. Make a release a fist (this can be done with your hands elevated). You could also squeeze a stress ball:
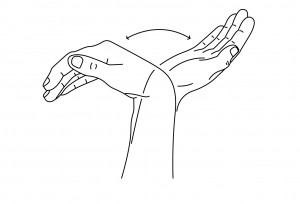
 3. Fingers bend and straighten. Forearm upright, wrist and fingers straight. Now hook your fingers down, trying to touch the tips of your fingers to the top of your palm. Straighten again. Repeat 10 times:
3. Fingers bend and straighten. Forearm upright, wrist and fingers straight. Now hook your fingers down, trying to touch the tips of your fingers to the top of your palm. Straighten again. Repeat 10 times:
