
Listeriosis
 Altough rare, listeriosis infection in pregnancy can lead to miscarriage, stillbirth or severe illness in newborn babies. Listeria can be found in unpasteurised milk and in many chilled foods including pâté.
Altough rare, listeriosis infection in pregnancy can lead to miscarriage, stillbirth or severe illness in newborn babies. Listeria can be found in unpasteurised milk and in many chilled foods including pâté.
Altough rare, listeriosis infection in pregnancy can lead to miscarriage, stillbirth or severe illness in newborn babies. Listeria can be found in unpasteurised milk and in many chilled foods including pâté.
Altough rare, listeriosis infection in pregnancy can lead to miscarriage, stillbirth or severe illness in newborn babies. Listeria can be found in unpasteurised milk and in many chilled foods including pâté.
 Chest pain in pregnancy and/or afer your baby’s birth should never be ignored. Some chest pain can be serious and can lead to a heart attack, heart failure, cardiac arrest or even death. Most women do not suffer from these conditions during or after pregnancy but it is important to recognise the symptoms and, if you have any of them, to seek treatment quickly.
Chest pain in pregnancy and/or afer your baby’s birth should never be ignored. Some chest pain can be serious and can lead to a heart attack, heart failure, cardiac arrest or even death. Most women do not suffer from these conditions during or after pregnancy but it is important to recognise the symptoms and, if you have any of them, to seek treatment quickly.
 SCAD is a rare but serious heart condition that causes a tear or bruise to develop in a coronary (heart) artery resulting in a blockage that prevents normal blood flow. It can cause heart attack, heart failure or cardiac arrest and can be fatal.
SCAD can happen during pregnancy and during the weeks and months after you have given birth. Symptoms can include:
SCAD is a rare but serious heart condition that causes a tear or bruise to develop in a coronary (heart) artery resulting in a blockage that prevents normal blood flow. It can cause heart attack, heart failure or cardiac arrest and can be fatal.
SCAD can happen during pregnancy and during the weeks and months after you have given birth. Symptoms can include:




 You can also do this exercise lying on your side, or when sitting or standing.
You can exercise this muscle effectively when you are walking around or lifting and carrying. Just draw your tummy in as if you were hugging your bump or wearing a bikini!
You can also do this exercise lying on your side, or when sitting or standing.
You can exercise this muscle effectively when you are walking around or lifting and carrying. Just draw your tummy in as if you were hugging your bump or wearing a bikini!
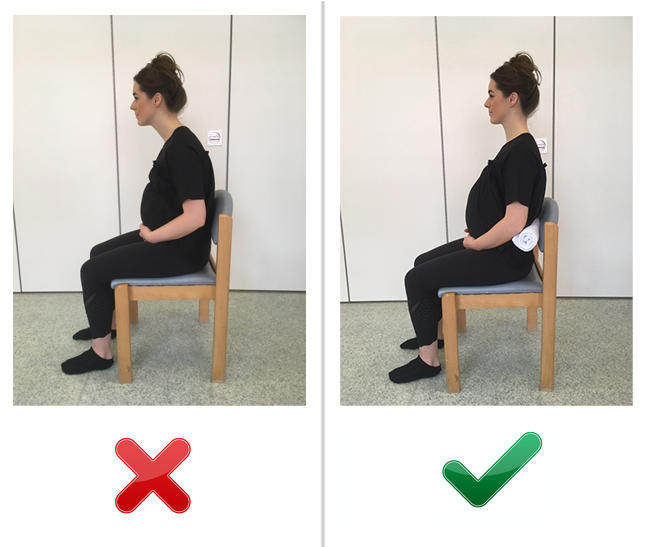
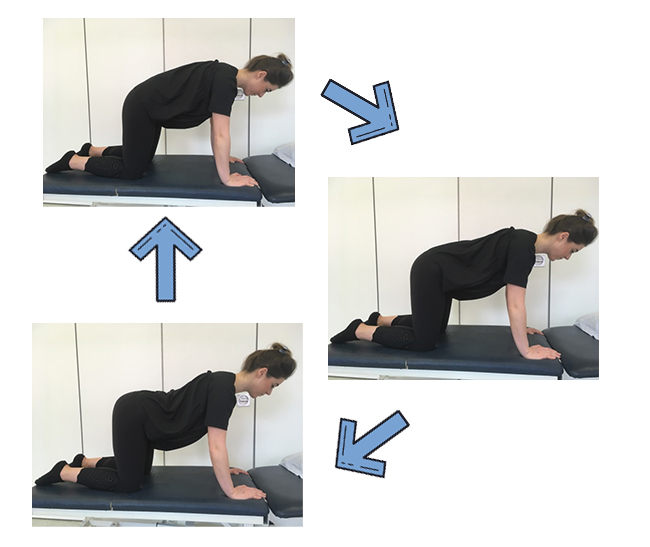
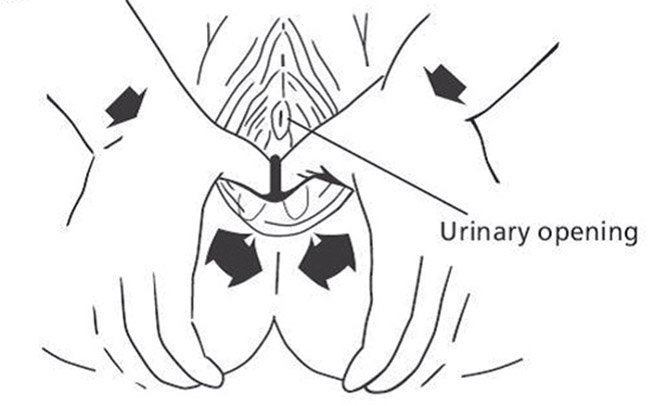
 Alternatively, you can try doing this exercise in different positions, such as when kneeling, leaning on the bed, sitting (on a chair or exercise ball), or on all fours) see pictures 1-2 and a-c).
Alternatively, you can try doing this exercise in different positions, such as when kneeling, leaning on the bed, sitting (on a chair or exercise ball), or on all fours) see pictures 1-2 and a-c).
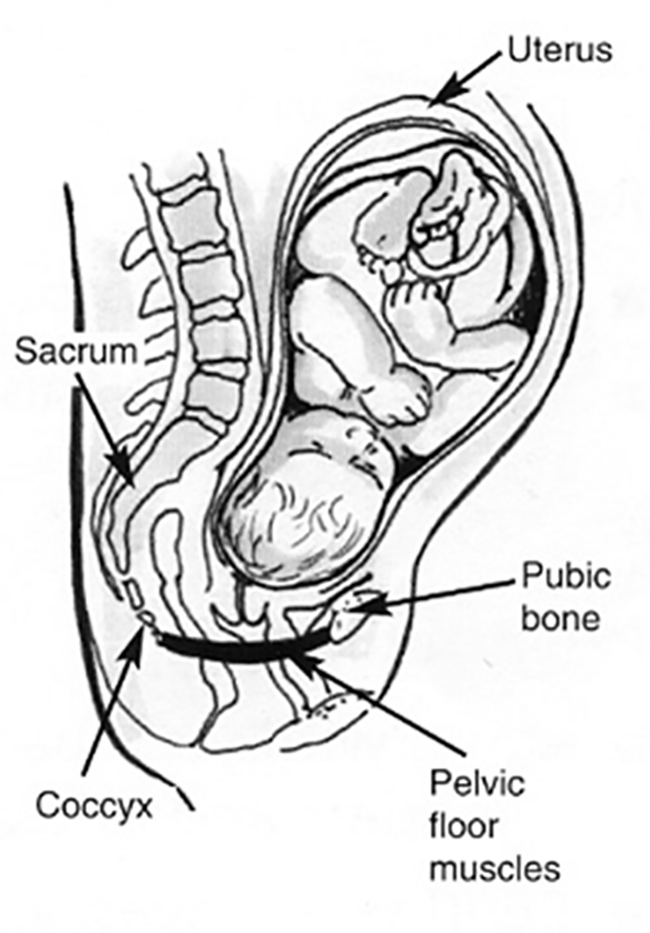 Some women may experience leakage of urine when coughing and sneezing (known as ‘stress urinary inconinence’) as a result of weak pelvic floor muscles. This is a common complaint affecting one in three women, but it can be prevented, reduced and even resolved fully with regular pelvic floor exercises.
It is highly recommended that all pregnant and postnatal women regularly exercise their pelvic floor muscles even if they have no problems with bladder control, to prevent problems in the future.
To begin with, you may have to concentrate while doing the exercises, but as you become more confident, you could do them whilst watching television, standing in a supermarket queue or waiting for the kettle to boil.
Some women may experience leakage of urine when coughing and sneezing (known as ‘stress urinary inconinence’) as a result of weak pelvic floor muscles. This is a common complaint affecting one in three women, but it can be prevented, reduced and even resolved fully with regular pelvic floor exercises.
It is highly recommended that all pregnant and postnatal women regularly exercise their pelvic floor muscles even if they have no problems with bladder control, to prevent problems in the future.
To begin with, you may have to concentrate while doing the exercises, but as you become more confident, you could do them whilst watching television, standing in a supermarket queue or waiting for the kettle to boil.
 Remember – it is not usually the one time we lift awkwardly or stand badly that causes pain; it is often the continual stresses and strains we place on our body during our everyday activities.
Therefore, it is important to modify your daily activities using the techniques in this booklet, do some of the gentle exercises we suggest and ensure you pace your activities throughout the day and week.
Please ask your midwife or GP to refer you to a physiotherapist if you are still having difficulties with pain.
Remember – it is not usually the one time we lift awkwardly or stand badly that causes pain; it is often the continual stresses and strains we place on our body during our everyday activities.
Therefore, it is important to modify your daily activities using the techniques in this booklet, do some of the gentle exercises we suggest and ensure you pace your activities throughout the day and week.
Please ask your midwife or GP to refer you to a physiotherapist if you are still having difficulties with pain.
 Following this, apply a firm pressure at 5, 6 and 7 on the imaginary clock. Hold each stretch until you feel a burning, stinging sensation for approximately 2 minutes. This technique may be painful/cause stinging sensation – this is normal.
Try working in a circular montion with your thumb or fingertip across the scar and concentrate on one area of the scar at a time. Begin with a gentle pressure and build up as you feel comfortable.
Massage can also be performed in the bath without addition of any oils.
Following this, apply a firm pressure at 5, 6 and 7 on the imaginary clock. Hold each stretch until you feel a burning, stinging sensation for approximately 2 minutes. This technique may be painful/cause stinging sensation – this is normal.
Try working in a circular montion with your thumb or fingertip across the scar and concentrate on one area of the scar at a time. Begin with a gentle pressure and build up as you feel comfortable.
Massage can also be performed in the bath without addition of any oils.

 Infection in pregnancy and/or after your baby’s birth should never be ignored. Some infections can progress to a more serious situation known as sepsis, where the infection spreads to the blood stream and through the whole body. If left untreated sepsis can lead to shock, organ failure and death. Whilst most women do not suffer from infection or sepsis during or after pregnancy, it needs to be recognised and treated quickly if they do.
Infection in pregnancy and/or after your baby’s birth should never be ignored. Some infections can progress to a more serious situation known as sepsis, where the infection spreads to the blood stream and through the whole body. If left untreated sepsis can lead to shock, organ failure and death. Whilst most women do not suffer from infection or sepsis during or after pregnancy, it needs to be recognised and treated quickly if they do.


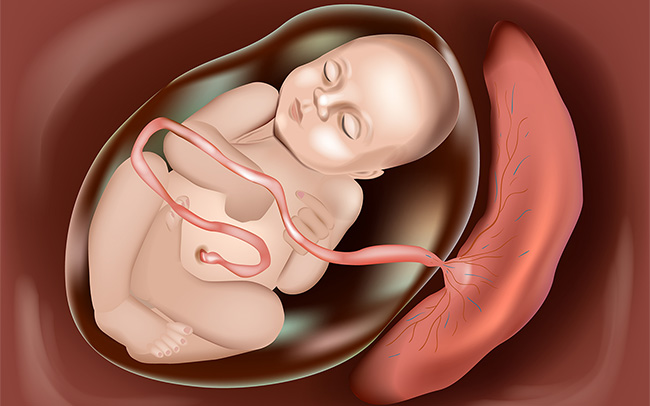 The placenta can also sometimes implant abnormally into the wall of the womb. This is a rare condition known as placenta accreta. The risk of having placenta accreta is higher if there is a previous scar on the womb, such as from a previous caesarean section, as the placenta can invade into the previous scar. This is a very serious condition that can be challenging to manage and a hysterectomy (operation to remove the womb) is sometimes needed at the time of delivery.
The placenta can also sometimes implant abnormally into the wall of the womb. This is a rare condition known as placenta accreta. The risk of having placenta accreta is higher if there is a previous scar on the womb, such as from a previous caesarean section, as the placenta can invade into the previous scar. This is a very serious condition that can be challenging to manage and a hysterectomy (operation to remove the womb) is sometimes needed at the time of delivery.
 This can be picked up on an ultrasound scan as a low lying placenta in mid pregnancy. This is when the placenta is covering all or part of the entrance to the womb.
If you are found to have a low lying placenta you will be rescanned between 32-36 weeks. The majority of low lying placentas will move to the upper part of the womb by 36 weeks, however 10% of low lying placentas remain low. This can cause bleeding in pregnancy that is sudden and severe. A caesarean birth may be recommended in cases of severe placenta praevia, and the likelihood of needing a blood transfusion can be higher.
This can be picked up on an ultrasound scan as a low lying placenta in mid pregnancy. This is when the placenta is covering all or part of the entrance to the womb.
If you are found to have a low lying placenta you will be rescanned between 32-36 weeks. The majority of low lying placentas will move to the upper part of the womb by 36 weeks, however 10% of low lying placentas remain low. This can cause bleeding in pregnancy that is sudden and severe. A caesarean birth may be recommended in cases of severe placenta praevia, and the likelihood of needing a blood transfusion can be higher.
 This is a liver disorder that can develop in pregnancy, usually after 30 weeks gestation, but which sometimes develop as early as 8 weeks, affecting up to one in every 140 pregnant women.
Symptoms can include:
This is a liver disorder that can develop in pregnancy, usually after 30 weeks gestation, but which sometimes develop as early as 8 weeks, affecting up to one in every 140 pregnant women.
Symptoms can include: